|
Overview
 The loss of the arch of the foot (also known in some cases as the ?instep?) is called a flatfoot. People may have a very low arch or absolutely no arch whatsoever. Whilst most people with flat feet have been that way since a young age, in some people the arch height reduces over time. This can be due to systemic health concerns, degeneration of muscles and joints, hormonal changes or specific injury. Causes Abnormal development of the foot, producing Pes Planus, may be due to neurological problems, eg cerebral palsy, polio. Bony or ligamentous abnormalities, eg tarsal coalition (fusion of tarsal bones), accessory navicular bone. A small proportion of flexible flat feet do not correct with growth. Some of these may become rigid if the Pes Planus leads to bony changes. Symptoms The primary symptom of flatfeet is the absence of an arch upon standing. Additional signs of flatfeet include the following. Foot pain. Pain or weakness in the lower legs. Pain or swelling on the inside of the ankle. Uneven shoe wear. While most cases of flatfeet do not cause problems, complications can sometimes occur. Complications include the following, bunions and calluses, inability to walk or run normally, inflammation and pain in the bottom of the foot (plantar fasciitis), tendonitis in the Achilles heel and other ligaments, pain in the ankles, knees, and hips due to improper alignment, shin splints, stress fractures in the lower legs. Diagnosis Most children and adults with flatfeet do not need to see a physician for diagnosis or treatment. However, it is a good idea to see a doctor if the feet tire easily or are painful after standing, it is difficult to move the foot around or stand on the toes, the foot aches, especially in the heel or arch, and there is swelling on the inner side of the foot, the pain interferes with activity or the person has been diagnosed with rheumatoid arthritis. Most flatfeet are diagnosed during physical examination. During the exam, the foot may be wetted and the patient asked to stand on a piece of paper. An outline of the entire foot will indicate a flattened arch. Also, when looking at the feet from behind, the ankle and heel may appear to lean inward (pronation). The patient may be asked to walk so the doctor can see how much the arch flattens during walking. The doctor may also examine the patient's shoes for signs of uneven wear, ask questions about a family history of flatfeet, and inquire about known neurological or muscular diseases. Imaging tests may be used to help in the diagnosis. If there is pain or the arch does not appear when the foot is flexed, x-rays are taken to determine the cause. If tarsal coalition is suspected, computed tomography (CT scan) may be performed, and if an injury to the tendons is suspected, magnetic resonance imaging (MRI scan) may be performed. Is flat footedness genetic? Non Surgical Treatment Treatment of flat feet by a fully educated, trained, and licensed podiatrist should be sought if the previously mentioned pain in the foot or knee areas start to surface and becomes a painful problem. Depending on the cause and exact type of the condition, a variety of forms of treatment may be prescribed. Verification of the exact cause and type of flat feet that each individual has, should only be handled by a professional podiatrist. Often times, the actual treatment method will include some form of arch support or light gymnastic style exercise. In rare cases, something more involved may be necessary, but only your skilled podiatrist would be able to accurately make that determination. If you suffer from flat feet, plantar fasciitis, or any other form of problematic foot condition, we encourage you to contact a foot clinic today and potentially rid yourself of that problem in virtually no time at all. Surgical Treatment  Procedures may include the following. Fusing foot or ankle bones together (arthrodesis). Removing bones or bony growths, also called spurs (excision). Cutting or changing the shape of the bone (osteotomy). Cleaning the tendons' protective coverings (synovectomy). Adding tendon from other parts of your body to tendons in your foot to help balance the "pull" of the tendons and form an arch (tendon transfer). Grafting bone to your foot to make the arch rise more naturally (lateral column lengthening). Overview
leg length discrepancy can be present from birth (congenital) or acquired (a result of an injury, infection or tumor). Some of the conditions that can cause limb problems in a child or young adult include congenital conditions present from birth. Osteogenesis imperfecta,. Bow legs. Knock knees. Neurofibromatosis. Arthritis. Infections of the bones and tumors. Injuries involving the growth center of the bone. There may also be deformities that are a result of the soft tissues and not the bones, such as with arthrogryposis and burns.  Causes Some children are born with absence or underdeveloped bones in the lower limbs e.g., congenital hemimelia. Others have a condition called hemihypertrophy that causes one side of the body to grow faster than the other. Sometimes, increased blood flow to one limb (as in a hemangioma or blood vessel tumor) stimulates growth to the limb. In other cases, injury or infection involving the epiphyseal plate (growth plate) of the femur or tibia inhibits or stops altogether the growth of the bone. Fractures healing in an overlapped position, even if the epiphyseal plate is not involved, can also cause limb length discrepancy. Neuromuscular problems like polio can also cause profound discrepancies, but thankfully, uncommon. Lastly, Wilms? tumor of the kidney in a child can cause hypertrophy of the lower limb on the same side. It is therefore important in a young child with hemihypertrophy to have an abdominal ultrasound exam done to rule out Wilms? tumor. It is important to distinguish true leg length discrepancy from apparent leg length discrepancy. Apparent discrepancy is due to an instability of the hip, that allows the proximal femur to migrate proximally, or due to an adduction or abduction contracture of the hip that causes pelvic obliquity, so that one hip is higher than the other. When the patient stands, it gives the impression of leg length discrepancy, when the problem is actually in the hip. Symptoms The effects of limb length discrepancy vary from patient to patient, depending on the cause and size of the difference. Differences of 3 1/2 percent to 4 percent of the total length of the leg (about 4 cm or 1 2/3 inches in an average adult) may cause noticeable abnormalities when walking. These differences may require the patient to exert more effort to walk. There is controversy about the effect of limb length discrepancy on back pain. Some studies show that people with a limb length discrepancy have a greater incidence of low back pain and an increased susceptibility to injuries. Other studies do not support this finding. Diagnosis There are several orthopedic tests that are used, but they are rudimentary and have some degree of error. Even using a tape measure with specific anatomic landmarks has its errors. Most leg length differences can be seen with a well trained eye, but I always recommend what is called a scanagram, or a x-ray bone length study (see picture above). This test will give a precise measurement in millimeters of the length difference. Non Surgical Treatment The key to treatment of LLD in a child is to predict what the discrepancy is at maturity. If it is predicted to be less than 2 cm., no treatment is needed. Limb length discrepancies of up to 2 or 2.5 cm. can be compensated very well with a lift in the shoe. Beyond 2.5 cm., it becomes increasingly difficult to compensate with a left in the insole. Building up the shoe becomes uncosmetic and cumbersome, and some other way of compensating for the discrepancy becomes necessary. The treatment of LLD is long-term treatment, and involves the physician and patient?s family working together as a team. The family needs to weigh the various options available. If leg lengthening is decided on, the family needs to understand the commitment necessary to see it through. The treatment takes 6 months to a year for completion, and complications can happen. But when it works, the results are gratifying.  how to grow taller at 17 Surgical Treatment Surgeries to lengthen a leg are generally only performed when there is a difference in leg length of greater than four centimeters. These types of surgeries can be more difficult and have more complications, such as infections, delayed healing, dislocations, and high blood pressure. In a several step process, bone lengthening surgeries involve cutting a bone in two in order to allow new bone growth to occur. After the bone is cut, a special apparatus is worn with pins that will pull the bone apart at approximately one millimeter per day. This causes osteogenesis, or new bone growth, in between the cut bone segments. A cast or brace may be required for several months after surgery to allow the new bone growth to harden and provide extra support. Overview
 Many types of heel pain are simply the result of overuse injuries and can easily be avoided. Follow these tips to reduce your chances of heel pain. Wear properly fitting shoes with good arch support. Replace them regularly. Stretch your feet, ankles, and legs before and after you exercise. Avoid walking barefoot on hard surfaces. If your feet hurt, stop what you?re doing. No pain is normal. Keep your weight under control, being overweight or obese can be a significant contributor to heel pain. Causes Rheumatoid arthritis and other forms of arthritis, including gout, which usually manifests itself in the big toe joint, can cause heel discomfort in some cases. Heel pain may also be the result of an inflamed bursa (bursitis), a small, irritated sack of fluid behind the heel. A neuroma (a nerve growth) involving the so-called Baxter's Nerve, (a nerve that courses under the heel bone), may also cause heel pain that mimics the pain of a heel spur. Tarsal Tunnel Syndrome, a pinched nerve beneath the inside ankle bone, too, can cause pain in the heel. Haglund's deformity ("pump bump") is a bone enlargement at the back of the heel bone, in the area where the Achilles tendon attaches to the bone. This sometimes painful deformity generally is the result of bursitis caused by pressure against the shoe, and can be aggravated by the height or stitching of a heel counter of a particular shoe. Pain at the back of the heel is associated with inflammation of the Achilles tendon as it runs behind the ankle and inserts on the back surface of the heel bone. The inflammation is called Achilles tendinitis. It is common among people who run and walk a lot and have tight tendons. The condition occurs when the tendon is strained over time, causing the fibbers to tear or stretch along its length, or at its insertion on to the heel bone. This leads to inflammation, pain, and the possible growth of a bone spur on the back of the heel bone. The inflammation is aggravated by the chronic irritation that sometimes accompanies an active lifestyle and certain activities that strain an already tight tendon. Bone bruises (Periostitis), are also common heel injuries. A bone bruise or contusion is an inflammation of the tissues that cover the heel bone. A bone bruise is a sharply painful injury caused by the direct impact of a hard object or surface on the foot. Stress fractures of the heel bone also can occur, but these are less frequent. On very rare occasions, there can be problems within the bone structure itself that cause heel pain. Paget's disease, cysts, bone tumours, and other conditions can occur in the heel causing pain, so it is important to be examined thoroughly. Symptoms Pain in the bottom of the heel is the most common symptom. The pain is often described as a knife-like, pinpoint pain that is worse in the morning and generally improves throughout the day. By the end of the day the pain may be replaced by a dull ache that improves with rest. The pain results from stretching the damaged tissues. For the same reason atheletes' pain occurs during beginning stages of exercise and is relieved over time as warm-up loosens the fascia. Plantar fasciitis onset is usually gradual, only flaring up during exercise. If pain is ignored, it can eventually interfere with walking and overall, plantar fasciitis accounts for about ten percent of all running injuries. Diagnosis In most cases, your GP or a podiatrist (a specialist in foot problems and foot care) should be able to diagnose the cause of your heel pain by asking about your symptoms and medical history, examining your heel and foot. Non Surgical Treatment Treatment options for plantar fasciitis include custom prescription foot orthoses (orthotics), weight loss when indicated, steroid injections and physical therapy to decrease the inflammation, night-splints and/or cast boots to splint and limit the stress on the plantar fascia. Orthotripsy (high frequency ultra-sonic shock waves) is also a new treatment option that has been shown to decrease the pain significantly in 50 to 85 percent of patients in published studies. Surgery, which can be done endoscopically, is usually not needed for over 90 percent of the cases of plantar fasciitis. (However, when surgery is needed, it is about 85 percent successful.) Patients who are overweight do not seem to benefit as much from surgery. Generally, plantar fasciitis is a condition people learn to control. There are a few conditions similar to plantar fascia in which patients should be aware. The most common is a rupture of the plantar fascia: the patient continues to exercise despite the symptoms and experiences a sudden sharp pain on the bottom of the heel and cannot stand on his or her toes, resulting in bruising in the arch. Ruptures are treated very successfully by immobilization in a cast boot for two to six weeks, a period of active rest and physical therapy. Another problem with prolonged and neglected plantar fasciitis is development of a stress fracture from the constant traction of this ligament on the heel bone. This appears more common in osteoporotic women, and is also treated with cast boot immobilization. The nerves that run along the heel occasionally become inflamed by the subsequent thickening and inflammation of the adjacent plantar fascia. These symptoms often feel like numbness and burning and usually resolve with physical therapy and injections. Patients should also be aware that heel numbness can be the first sign of a back problem. Surgical Treatment With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick. heel pads shoes too big Prevention  Preventing heel pain is crucial to avoid pain that can easily interrupt a busy or active lifestyle. Athletes can prevent damage by stretching the foot and calf both before and after an exercise routine. The plantar fascia ligament can be stretched by using a tennis ball or water bottle and rolling it across the bottom of the foot. With regular stretching, the stretching and flexibility of tissue through the foot can be significantly improved, helping to prevent damage and injury. Athletes should also ease into new or more difficult routines, allowing the plantar fascia and other tissue to become accustomed to the added stress and difficulty. Running up hills is also common among athletes in their routines. However, this activity should be reduced since it places an increased amount of stress on the plantar fascia and increases the risk of plantar fasciitis. Maintaining a healthy weight is also an essential heel pain prevention technique. Obesity brings additional weight and stress on the heel of the foot, causing damage and pain in the heel as well as in other areas of the foot. Overview
 A morton's neuroma (or an "inter-digital" neuroma) is found between the toes of the foot, most commonly the third and fourth toes. It can also occur between the metatarsal bones (the long bones in the forefoot). It is basically an entrapped nerve, which becomes inflamed due to constant irritation from the surrounding bony structures. A morton's neuroma (or an "inter-digital" neuroma) is found between the toes of the foot, most commonly the third and fourth toes. It can also occur between the metatarsal bones (the long bones in the forefoot). It is basically an entrapped nerve, which becomes inflamed due to constant irritation from the surrounding bony structures.Causes The source of this pain is an enlargment of the sheath of an intermetatarsal nerve in the foot. This usually occurs in the third intermetatarsal space, the space between the third and fourth toes and metatarsals. It occurs here, at the site third intermetatarsal nerve, since this intermetatarsal nerve is the thickest being comprised of the joining of two different nerves. It also may occur in the other intermetatarsal areas, with the second interspace being the next most common location. Symptoms Symptoms typically include pain, often with pins and needles on one side of a toe and the adjacent side of the next toe. Pain is made worse by forefoot weight bearing and can also be reproduced by squeezing the forefoot to further compress the nerve. Pressing in between the third and forth metatarsals for example with a pen can also trigger symptoms. Diagnosis During the exam, your doctor will press on your foot to feel for a mass or tender spot. There may also be a feeling of "clicking" between the bones of your foot. Some imaging tests are more useful than others in the diagnosis of Morton's neuroma. Your doctor is likely to order X-rays of your foot, to rule out other causes of your pain such as a stress fracture. Ultrasound. This technology uses sound waves to create real-time images of internal structures. Ultrasound is particularly good at revealing soft tissue abnormalities, such as neuromas. Magnetic resonance imaging (MRI). Using radio waves and a strong magnetic field, an MRI also is good at visualizing soft tissues. But it's an expensive test and often indicates neuromas in people who have no symptoms. Non Surgical Treatment The best results are achieved with massage techniques that encourage spreading and mobilizing the metatarsal heads. Metatarsal spreading is one technique that can help reduce the detrimental effects of nerve compression. To perform this technique, pull the metatarsal heads (not just the toes) apart and hold them in this position to help stretch the intrinsic foot muscles and other soft-tissues. When this technique is combined with the use of toe spacers, it will be even more effective.  Surgical Treatment Surgery for Morton's neuroma is usually a treatment of last resort. It may be recommended if you have severe pain in your foot or if non-surgical treatments haven't worked. Surgery is usually carried out under local anaesthetic, on an outpatient basis, which means you won't need to stay in hospital overnight. The operation can take up to 30 minutes. The surgeon will make a small incision, either on the top of your foot or on the sole. They may try to increase the space around the nerve (nerve decompression) by removing some of the surrounding tissue, or they may remove the nerve completely (nerve resection). If the nerve is removed, the area between your toes may be permanently numb. After the procedure you'll need to wear a special protective shoe until the affected area has healed sufficiently to wear normal footwear. It can take up to four weeks to make a full recovery. Most people (about 75%) who have surgery to treat Morton's neuroma have positive results and their painful symptoms are relieved.  Overview OverviewA Hammertoes is a toe that is bent because of a weakened muscle. The weakened muscle makes the tendons (tissues that connect muscles to bone) shorter, causing the toes to curl under the feet. Hammertoes can run in families. They can also be caused by shoes that are too short. Hammertoes can cause problems with walking and can lead to other foot problems, such as blisters, calluses, and sores. Splinting and corrective footwear can help in treating hammertoes. In severe cases, surgery to straighten the toe may be necessary. Causes Wearing ill-fitting shoes is probably the main cause of hammer toe. As the toe bends, tendons add to the problem by contracting in such a way that the bending is reinforced to the point of becoming permanent. In some cases, tendons that are abnormal to begin with may start the bending process.  Symptoms A soft corn, or heloma molle, may exist in the web space between toes. This is more commonly caused by an exostosis, which is basically an extra growth of bone possibly due to your foot structure. As this outgrowth of excessive bone rubs against other toes, there is friction between the toes and a corn forms for your protection. Diagnosis Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. Non Surgical Treatment You can usually use over-the-counter cushions, pads, or medications to treat bunions and corns. However, if they are painful or if they have caused your toes to become deformed, your doctor may opt to surgically remove them. If you have blisters on your toes, do not pop them. Popping blisters can cause pain and infection. Use over-the-counter creams and cushions to relieve pain and keep blisters from rubbing against the inside of your shoes. Gently stretching your toes can also help relieve pain and reposition the affected toe. Surgical Treatment If your hammer, claw, or mallet toe gets worse, or if nonsurgical treatment does not help your pain, you may think about surgery. The type of surgery you choose depends on how severe your condition is and whether the toe joint is fixed (has no movement) or flexible (has some movement). A fixed toe joint often requires surgery to be straightened. A flexible toe joint can sometimes be straightened without surgery. Surgery choices include Phalangeal head resection (arthroplasty), in which the surgeon removes part of the toe bone. Joint fusion (arthrodesis), in which the surgeon removes part of the joint, letting the toe bones grow together (fuse). Cutting supporting tissue or moving tendons in the toe joint. How well surgery works depends on what type of surgery you have, how experienced your surgeon is, and how badly your toes are affected.  Overview Overviewhammertoe is a secondary problem originating from fallen cross arches. The toes start to curl and get pulled backwards, as the collapsed or pushed out metatarsal bones pull the tendons and ligaments, and causes them to get shorter and tighter. This condition causes the toes have higher pressure and they have limited movement and cannot be straightened fully. This can lead to numbness and pain in the toes as muscles, nerves, joints and little ligaments are involved with this condition. As the top part of the toe can rub against the shoe, it can cause corns and calluses. Causes The muscles of each toe work in pairs. When the toe muscles get out of balance, a hammer toe can form. Muscle imbalance puts a lot of pressure on the toe's tendons and joints. This pressure forces the toe into a hammerhead shape. How do the toe muscles get out of balance? There are three main reasons. Your genes, you may have inherited a tendency to develop hammer toes because your foot is slightly unstable - such as a flat foot. But high-arched feet can also get hammer toes. Arthritis. Injury to the toe: ill-fitting shoes are the main culprits of this cause. If shoes are too tight, too short, or too pointy, they push the toes out of balance. Pointy, high-heeled shoes put particularly severe pressure on the toes.  Symptoms SymptomsCommon reasons patients seek treatment for toe problems are toe pain on the knuckle. Thick toe calluses. Interference with walking/activities. Difficulty fitting shoes. Worsening toe deformity. Pain at the ball of the foot. Unsightly appearance. Toe deformities (contractures) come in varying degrees of severity, from slight to severe. The can be present in conjunction with a bunion, and develop onto a severe disfiguring foot deformity. Advanced cases, the toe can dislocate on top of the foot. Depending on your overall health, symptoms and severity of the hammer toe, the condition may be treated conservatively and/or with surgery. Diagnosis Some questions your doctor may ask of you include, when did you first begin having foot problems? How much pain are your feet or toes causing you? Where is the pain located? What, if anything, seems to improve your symptoms? What, if anything, appears to worsen your symptoms? What kind of shoes do you normally wear? Your doctor can diagnose hammertoe or mallet toe by examining your foot. Your doctor may also order X-rays to further evaluate the bones and joints of your feet and toes. Non Surgical Treatment If the toes are still mobile enough that they are able to stretch out and lay flat, the doctor will likely suggest a change of footwear. In addition, she may choose to treat the pain that may result from the condition. The doctor may prescribe pads to ease the pain of any corns and calluses, and medications ranging from ibuprofen to steroid injections for the inflammation and pain. Other options for non-surgical treatments include orthotic devices to help with the tendon and muscle imbalance or splinting to help realign the toe. Splinting devices come in a variety of shapes and sizes but the purpose of each is the same: to stretch the muscles and tendon and flatten the joint to remove the pain and pressure that comes from corns. Surgical Treatment Surgically correcting a hammertoe is very technical and difficult, and requires a surgeon with superior capabilities and experience. The operation can be done at our office or the hospital with local anesthetic. After making a small incision, the deformity is reduced and the tendons are realigned at the joint. You will be able to go home the same day with a special shoe! If you are sick and tired of not fitting your shoes, you can no longer get relief from pads, orthopedic shoes or pedicures, and have corns that are ugly, sensitive and painful, then you certainly may be a good surgical candidate. In order to have this surgery, you can not have poor circulation and and must have a clean bill of health.  Prevention PreventionPrevention of a hammertoe can be difficult as symptoms do not arise until the problem exists. Wearing shoes Hammer toe that have extra room in the toes may eliminate the problem or slow down the deformity from getting worse. Sometimes surgery is recommended for the condition. If the area is irritated with redness, swelling, and pain some ice and anti-inflammatory medications may be helpful. The best prevention may be to get advice from your podiatrist. Overview
Pronation is the normal movement the foot makes to absorb the impact from walking or running. It occurs once the heel strikes the ground and the foot disperses the impact, stretching and flattening the arch as the foot rolls inward. Supination is the opposite motion of pronation. The foot supinates, or rolls on its outer edge, to help with stability as we walk or run. A reasonable amount of pronation is necessary for the foot to function properly. However, when the foot arch remains flat and the foot rolls inward too much one may have excessive pronation or overpronation. This medical condition can result from continually straining the feet and wearing footwear that lacks sufficient foot arch support.  Causes Over-pronation may happen because the tissue that attaches to your foot bones is loose. You may be born with this problem or it may result from injuries or overuse, like from too much running. Symptoms Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses. Diagnosis To easily get an idea of whether a person overpronates, look at the position and condition of certain structures in the feet and ankles when he/she stands still. When performing weight-bearing activities like walking or running, muscles and other soft tissue structures work to control gravity's effect and ground reaction forces to the joints. If the muscles of the leg, pelvis, and feet are working correctly, then the joints in these areas such as the knees, hips, and ankles will experience less stress. However, if the muscles and other soft tissues are not working efficiently, then structural changes and clues in the feet are visible and indicate habitual overpronation.  Non Surgical Treatment Heel counters that make the heel of the shoe stronger to help resist/reduce excessive rearfoot motions. The heel counter is the hard piece in the back of the shoe that controls the foot?s motion from side-to-side. You can quickly test the effectiveness of a shoe?s heel counter by placing the shoe in the palm of your hand and putting your thumb in the mid-portion of the heel, trying to bend the back of the shoe. A heel counter that does not bend very much will provide superior motion control. Appropriate midsole density, the firmer the density, the more it will resist motion (important for a foot that overpronates or is pes planus), and the softer the density, the more it will shock absorb (important for a cavus foot with poor shock absorption) Wide base of support through the midfoot, to provide more support under a foot that is overpronated or the middle of the foot is collapsed inward. Surgical Treatment Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. Overview
Leg length discrepancy (LLD) affects about 70% of the general population, and can be either structural - when the difference occurs in bone structures - or functional, because of mechanical changes at the lower limbs. The discrepancy can be also classified by its magnitude into mild, intermediate, or severe. Mild LLD has been particularly associated with stress fracture, low back pain and osteoarthritis, and when the discrepancy occurs in subjects whose mechanical loads are increased by their professional, daily or recreational activities, these orthopaedic changes may appear early and severely. The aim of this study was to analyze and compare ground reaction force (GRF) during gait in runners with and without mild LLD. Results showed that subjects with mild LLD of 0.5 to 2.0 cm presented higher values of minimum vertical GRF (0.57 ? 0.07 BW) at the shorter limb compared to the longer limb (0.56 ? 0.08 BW) Therefore, subjects with mild LLD adopt compensatory mechanisms that cause additional overloads to the musculoskeletal system in order to promote a symmetrical gait pattern as showed by the values of absolute symmetric index of vertical and horizontal GRF variables.  Causes There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities. Symptoms As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies. Diagnosis The evaluation of leg length discrepancy typically involves sequential x-rays to measure the exact discrepancy, while following its progression. In addition, an x-ray of the wrist allows us to more carefully age your child. Skeletal age and chronological age do not necessarily equal each other and frequently a child's bone age will be significantly different than his or her stated age. Your child's physician can establish a treatment plan once all the facts are known: the bone age, the exact amount of discrepancy, and the cause, if it can be identified. Non Surgical Treatment To begin a path torwards a balanced foundation and reduce pain from leg length discrepancy, ask your doctor about these Functional Orthotics and procedures. Functional Orthotics have been shown to specifically reduce pain from leg length inequality, support all three arches of the foot to create a balanced foundation, maximize shock absorption, add extra propulsion, and supply more stability, enable posture correction and long-term preventive protection. Will improve prolonged effectiveness of chiropractic adjustments. Shoe or heel Lifts, Correct the deficiencies that causes imbalances in the body.  Surgical Treatment Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Overview
For many adults, years of wear and tear on the feet can lead to a gradual and potentially debilitating collapse of the arch. However, a new treatment approach based on early surgical intervention is achieving a high rate of longterm success. Based on results of clinical studies of adults with flat feet, we now believe that reconstructive surgery in the early stages of the condition can prevent complications later on. Left untreated, the arch eventually will collapse, causing debilitating arthritis in the foot and ankle. At this end stage, surgical fusions are often required to stabilize the foot.  Causes Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs. Symptoms Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. Asymmetrical collapsing of the medial arch on the affected side. Diagnosis Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered. Non surgical Treatment Flatfoot deformity can be treated conservatively or with surgical intervention depending on the severity of the condition. When people notice their arches flattening, they should immediately avoid non-supportive shoes such as flip-flops, sandals or thin-soled tennis shoes. Theses shoes will only worsen the flatfoot deformity and exacerbate arch pain. Next, custom orthotics are essential for people with collapsed arches. Over-the-counter insoles only provide cushion and padding to the arch, whereas custom orthotics are fabricated to specifically fit the patient?s foot and provide support in the arch where the posterior tibial tendon is unable to anymore. Use of custom orthotics in the early phases of flatfoot or PTTD can prevent worsening of symptoms and prevent further attenuation or injury to the posterior tibial tendon. In more severe cases of flatfoot deformity an ankle foot orthosis (AFO) such as a Ritchie brace is needed. This brace provides more support to the arch and hindfoot rather than an orthotic but can be bulky in normal shoegear. Additional treatment along with use of custom orthotics is use of non-steroidal anti-inflammatories (NSAIDS) such as Advil, Motrin, or Ibuprofen which can decrease inflammation to the posterior tibial tendon. If pain is severe, the patient may need to be placed in a below the knee air walker boot for several weeks which will allow the tendon to rest and heal, especially if a posterior tibial tendon tear is noted on MRI. 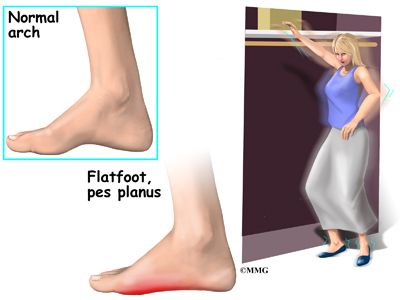 Surgical Treatment Until recently, operative treatment was indicated for most patients with stage 2 deformities. However, with the use of potentially effective nonoperative management , operative treatment is now indicated for those patients that have failed nonoperative management. The principles of operative treatment of stage 2 deformities include transferring another tendon to help serve the role of the dysfunctional posterior tibial tendon (usually the flexor hallucis longus is transferred). Restoring the shape and alignment of the foot. This moves the weight bearing axis back to the center of the ankle. Changing the shape of the foot can be achieved by one or more of the following procedures. Cutting the heel bone and shifting it to the inside (Medializing calcaneal osteotomy). Lateral column lengthening restores the arch and overall alignment of the foot. Medial column stabilization. This stiffens the ray of the big toe to better support the arch. Lengthening of the Achilles tendon or Gastrocnemius. This will allow the ankle to move adequately once the alignment of the foot is corrected. Stage 3 acquired adult flatfoot deformity is treated operatively with a hindfoot fusion (arthrodesis). This is done with either a double or triple arthrodesis - fusion of two or three of the joints in hindfoot through which the deformity occurs. It is important when a hindfoot arthrodesis is performed that it be done in such a way that the underlying foot deformity is corrected first. Simply fusing the hindfoot joints in place is no longer acceptable. |
